
If you’ve ever wondered how dentists decide what type of partial denture a patient needs, there’s a system behind it and it’s called Kennedy’s Classification. It’s one of the most important concepts in Prosthodontics, especially when planning Removable Partial Dentures (RPDs). The best part? Once you understand this system, designing or understanding RPDs becomes so much easier.
In this blog, we will explain Kennedy's classification system, where and how it is used in dentistry.
About Kennedy’s Classification
Dr. Edward Kennedy introduced Kennedy’s Classification in the 1920s as a simple and systematic way to classify partial edentulism (when a patient is missing some, but not all, teeth in an arch).
This system quickly became one of the most important concepts in Prosthodontics because it helps dentists plan and design Removable Partial Dentures (RPDs) with precision.
By applying Kennedy’s Classification, dental professionals can:
- Identify the pattern of missing teeth
- Choose the right RPD design for each situation
- Ensure the denture fits comfortably, functions efficiently, and looks natural
The Four Classes Of Kennedy's Classification
Kennedy’s system groups partial edentulism into four main classes, based on where the missing teeth are located. This gives dentists a structured way to plan treatment.
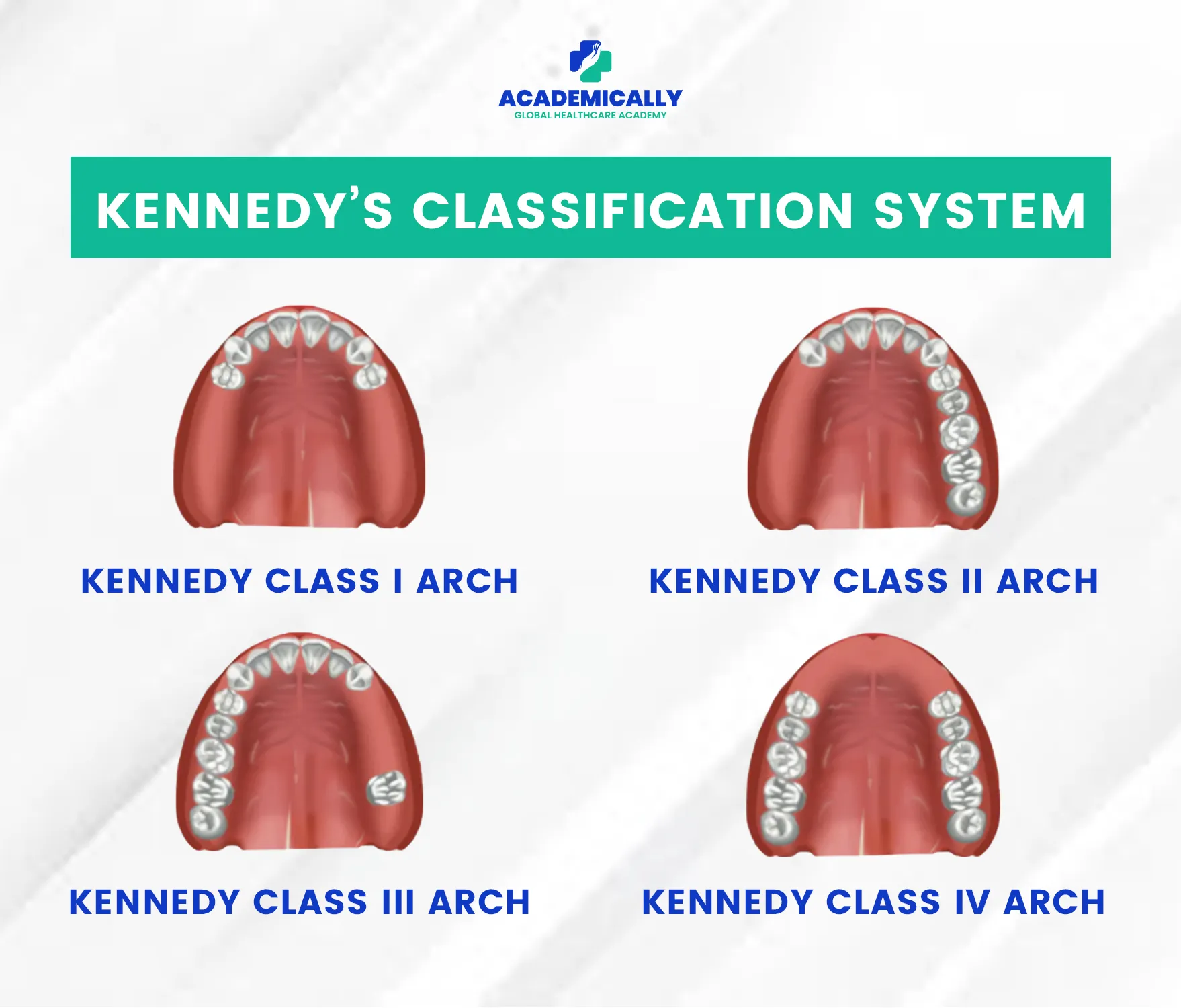
Class I
Class I includes bilateral edentulous areas that are located posterior to the remaining natural teeth. This means there are no natural teeth on either side at the back of the dental arch.
Example: Missing molars and premolars on the dental arch's left and right sides.
Considerations:
- Support is mainly taken from the remaining anterior teeth.
- Needs major connectors and indirect retainers to prevent shifting or rotation.
- Lack of posterior teeth makes retention and stability more challenging.
- May require precision attachments or implants for added support.
Class II
Class II consists of a unilateral edentulous area that is located posterior to the remaining natural teeth. This means that one side of the dental arch has no natural teeth at the back.
Example: The right side of the dental arch has missing molars and premolars, while the left side retains all teeth.
Considerations:
- Forces must be balanced on the edentulous side to avoid tilting and stress on remaining teeth.
- Often requires a stronger framework for stability and to prevent rotation.
- Clasps and indirect retainers are essential for retention and support.
- May include stress-breakers or flexible connectors to manage uneven force distribution.
Class III
Class III features a unilateral edentulous area with natural teeth remaining both anterior and posterior to it. This type of edentulous space is bounded by natural teeth on either side.
Example: There is a single gap on the left side of the dental arch, with natural teeth both in front of and behind the gap.
Considerations:
- Easier to design due to natural tooth support on both sides of the gap.
- Provides good stability and retention with minimal denture movement.
- Usually allows for a simple design with conventional clasp assemblies.
- Often no extra stabilising features are needed.
- Adjacent natural teeth help evenly distribute forces.
Class IV
Class IV is characterised by a single but bilateral (crossing the midline) edentulous area located anterior to the remaining natural teeth. This type involves the loss of front teeth.
Example: Missing central and lateral incisors, crossing the midline, while the canines and posterior teeth remain intact.
Considerations:
- Aesthetics are a priority because the missing teeth are highly visible.
- Requires careful planning for a natural look and proper function.
- Should include lifelike teeth and natural-looking gum for a seamless appearance.
- Needs good stability and retention, may use clasps, precision attachments, or implants.
- Aim is to blend with natural teeth for both cosmetic appeal and function.
| Class | Location of Missing Teeth | Support Challenge Level |
| Class I | Bilateral posterior | High |
| Class II | Unilateral posterior | Moderate–High |
| Class III | Single bounded area | Low |
| Class IV | Single anterior crossing midline | Moderate (mainly aesthetic) |
Preparing for the ADC exams? Kennedy’s Classification is a high-yield topic and frequently tested in Prosthodontics. Make sure you master the basics! Enroll in Academically’s ADC Preparation Course and crack the exam on the first attempt.
Applegate’s Rules for Applying Kennedy’s Classification
Now that you understand the four main classes, it’s important to know how to correctly apply this classification in real clinical situations. This is where Applegate’s Rules come in.
These rules help ensure that Kennedy’s Classification is used accurately when planning a Removable Partial Denture.
Here are Applegate’s 8 rules explained in a simple and easy-to-remember way:
| Rule No. | Applegate’s Rule |
| Rule 1 | Classification should be done after all necessary extractions. |
| Rule 2 | A missing 3rd molar is not considered if it is not going to be replaced. |
| Rule 3 | A present 3rd molar is considered if it will be used as an abutment. |
| Rule 4 | A missing 2nd molar is not considered if it is not going to be replaced. |
| Rule 5 | The most posterior edentulous area determines the classification. |
| Rule 6 | Additional edentulous areas apart from the main determining area are modification spaces. |
| Rule 7 | Only the number of modification spaces is counted, not the number of missing teeth. |
| Rule 8 | There are no modification spaces in Class IV. |
Struggling to remember all the rules and classifications for exams like the ADC?
In our ADC preparation course, we teach easy memory tricks, case-based examples, and exam-oriented ways to apply these concepts, so you don’t just memorise them, you understand them.
Importance of Kennedy’s Classification in Dental Practice
Kennedy’s Classification plays a vital role in diagnosis, treatment planning, and communication in dentistry. Here’s why it is so valuable:
- Improved Treatment Planning: Helps in designing functional, stable, and aesthetic RPDs tailored to the patient’s needs.
- Predictable Results: Supports better distribution of forces, comfort, and long-term success of the denture.
- Clear Communication: Provides a standard terminology for dentists, dental students, labs, and technicians.
Final Thoughts
Kennedy’s Classification is one of the most important systems in Prosthodontics for assessing partial edentulism and planning RPDs. It offers a clear, structured approach that helps design dentures which restore function, comfort, and a natural smile.
When combined with Applegate’s Rules, it allows for more accurate case classification and effective treatment planning, leading to better patient outcomes and improved oral function.
If you’d like to deepen your understanding of topics like this or need guidance for exams such as the ADC, our experts at Academically are here to support you.


